Cats
The size guide, copied below, is based on the ideal body weight of the patient. Ideally the largest size that can be safely inserted should be used. The inserted device should feel snug and should not move easily.

v-gel® devices are safe and appropriate for use during feline dental procedures. Such procedures are mainly performed on adult cats, so an appropriately sized v-gel® should be used chosen according to the size guide. The v-gel® should be securely tied in place to prevent rostral displacement. By sealing around, isolating the glottis aspiration of coolant water is much less likely to occur than with use of an endotracheal tube. The head should be positioned in a gentle downwards slope to encourage fluid to flow out of the mouth. Docsinnovent recommend the use of a d-grip® to support the circuit tubing.
v-gel® can safely and effectively be used for establishing and maintaining the patent airway of cats during anaesthesia or resuscitation. Cat v-gel® Advanced devices;
• are far easier and faster to place than an endotracheal tube with an airway being established in under 10 seconds.
• allow a trauma-free airway
• give an excellent seal – you can use lower gas flows and protect your staff against the hazards of leaking volatile anaesthetic agents.
• give the patient a much smoother recovery avoiding the risks of extubation laryngospasms and trauma
An endotracheal tube increases
• the risk of trauma to the upper airway structures and larynx. Trauma can result in post-operative glottic oedema resulting in morbidity (coughing, laryngospasm, bronchospasm, bleeding, sore throat, dysphagia, dysphonia, infection etc.) and mortality – gross glottic oedema can occasionally lead to airway obstruction resulting in death. Incidence of anaesthesia mortality in rabbits is about 1.69% and in cats about 1%, whilst in humans its 0.001%.
• the work of breathing especially for a spontaneous breathing patient, by reducing the internal diameter of the patient’s airway (trachea) by about 40%
• the risk of gas leakage into the atmosphere as uncuffed tubes have limited sealing capability against the trachea. This exposes staff to potentially toxic volatile anaesthetic agents, increases the cost of anaesthesia and means that your patient is getting suboptimal doses of anaesthetic agent
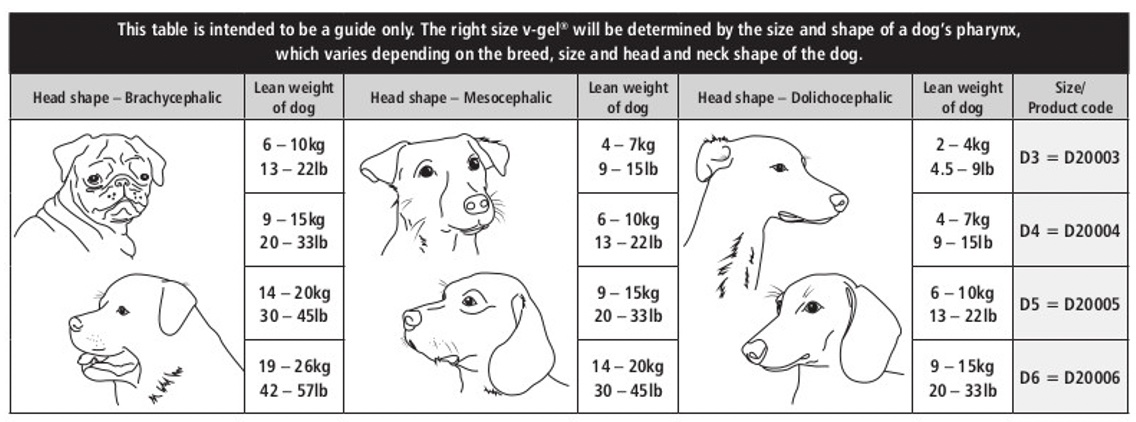
Dogs
Use the sizing guide which is based on the head shape and lean body weight of the patient. For meso- and dolicephalic breeds, if your patient is in between two different v-gel® sizes, it is generally better to pick the larger one. Brachycephalic dogs tend to have a small pharynx, so if in 2 size groups, pick the smaller of the two sizes.
This gastric channel allows passage of a tube through the v-gel® and into the oesophagus or stomach. Passage into the oesophagus allows identification of reflux as well as management through draining and flushing the oesophagus.
Yes, you can. The port will fit a 12Fr device, so slender probes and stethoscopes fit down the gastric channel very well. If the gastric channel is filled by these tubes, it will not work as effectively for drainage of gastric fluid although the v-gel® device will still isolate the airway from the oesophagus.
The channel will take devices up to 12Fr
No!
The gastric channel is designed to guide gastric fluid away from the patient’s upper airway If the airway is clear and your patient is breathing normally, just suction the gastric channel, oesophagus and/or stomach to remove any fluid or gastric material, then flush the oesophagus with sterile saline via the gastric channel until no more regurgitate is suctioned
Use of a v-gel® does not cause cilia trauma or increase airway resistance like endotracheal tubes do. It also offers more protection against reflux and regurgitation which are common complications in canine anaesthesia. An endotracheal tube offers little separation between the proximal trachea and oesophagus, when cuffed it offers some protection against regurgitate entering the distal trachea, however proximal exposure to regurgitated fluid is likely to cause mucosal trauma in the larynx and trachea.
Yes, the v-gel® is appropriate for most dental procedures. Once the v-gel® is in place, it should be securely tied in place to prevent rostral displacement. The isolation of the glottis will reduce the risk of aspiration of coolant fluid. as extra protection, the pharynx or caudal oral cavity should be packed with clean swabs. These swabs should be checked and changed frequently during the procedure. The head should be positioned in a gentle downwards slope to encourage fluid to flow out of the mouth. Docsinnovent recommend the use of a d-grip® to support the circuit tubing.
v-gel® should NOT be used in the following situations
Where access to the pharynx is required
- When a patient has received a neuromuscular block drug in protocol
- In patients with a compromised airway e.g. those suffering from collapsing trachea or laryngeal paralysis
- In patients where access to oesophagus is required eg passing of gastroscope
this is not a limitless list
There are many published papers on the incidence of both reflux and regurgitation. In dogs, reported incidence of reflux is over 70% in dogs (Raptopolous 2019, Rodriguez-Alarcon et al 2015). The incidence of regurgitation is up to 48% in dogs (Viskier and Sjöström 2017), leading to aspiration in 0.17% (Ovbey et al. 2014). Often these events are silent and not seen by the clinician until symptoms are seen after the patient has recovered from the anaesthesia.
Airway protection is vital and mild symptoms of oesophagitis may not be recognised by the owner. Oesophageal discomfort may influence the recovery of the patient. Being able to identify and safely manage reflux will improve patient status.
yes, v-gel® can be an appropriate device. for Brachycephalic breeds if these dogs have a functional larynx and trachea without anatomical defects such as laryngeal or tracheal collapse and access for BOAS surgery is not required. Some brachycephalic dogs can have abnormalities that are difficult to detect, such as loose laryngeal mucosa that can progressively block the airway, or abnormal epiglottis anatomy that can fold after v-gel® insertion to cause airway obstruction: the v-gel® should then be used with care in these cases.
Due to the placement of the v-gel® in the pharynx rather than through the larynx, it can be left in situ during recovery beyond the recommended removal of an endotracheal tube. This allows the patient to breathe either oxygen or room air with a secure airway for a longer period.
Rabbits
The size guide, copied below, is based on the ideal body weight of the patient. The largest device that can fit safely into the patient should be selected. Further assistance/advice can be found in the next question.
Once inserted, the device should feel snug and should not move easily.

Body weight is the most common used parameter when looking at anaesthesia: dosage rate, choice of anaesthesia circuit, tidal volume assessments, fresh gas flow calculations, however there are many times where body weight does not correlate completely to head size. Body weight is NOT the single determinant of v-gel® size selection: Head size, length and width of neck are also very important anatomical determinations when selecting the ideal size v-gel® devices for our patients.
The v-gel® sizing guide is a very good starting point using the adult ideal body weight but very young rabbits may require a larger size than expected.
Immature rabbits for anaesthesia, commonly for neutering, are often presented with a lighter body weight than perhaps their head size would suggest. So when considering correct size v-gel® for an immature patient, look at their head size and gauge what their ideal weight should be for the head size you are seeing in order to select the v-gel® from our size guide. You can also measure the oropharyngeal length, the distance between the larynx and incisors (following the line of the anatomical airway) and measure this against the length of the v-gel® (see image). The middle section of the pharyngeal bowl would lay level with the larynx and the incisors should lay on the airway channel just before its widens.

v-gel® devices are very useful for rabbit dentistry. They can be used for many routine and advanced procedures. Once the mouth is opened with a dental gag and cheek dilators, there is enough space around the v-gel® to examine and rasp/burr the molar teeth. The v-gel® can be flexed either side of the incisors allowing good access to the mouth. Docsinnovent recommend the use of a D-grip® to support the circuit tubing.
General
As the v-gel® doesn’t touch or travel through the arytenoids, the occurrence of laryngospasm is greatly reduced. Most serious spasms result from endotracheal intubation touching the sensitive areas of the upper airway.
However, laryngospasm can result from a painful stimulus if the patient is in a sub-optimal plane of anaesthesia. Therefore, users must ensure that the patient is at a surgical plane of anaesthesia and devices are adequately lubricated before inserting any airway device into their patient. If the user experiences a transient laryngospasm with the v-gel ® in situ, gently ventilating the patient while simultaneously deepening the plane of anaesthesia using an appropriate agent will resolve the spasm.
There is no contra indication is using a safe volume of lidocaine spray on the larynx 60-90 seconds prior to v-gel® insertion.
With the correct sized v-gel® in place, secured with a tie tightly behind the patient’s head, the design features of the v-gel® stabilises it; so that with normal turning and re-positioning, the v-gel® will not dislodge. The v-gel® should always be disconnected from the anaesthetic circuit, and the patient’s head supported, during repositioning. Always check the position and placement of your v-gel® after turning or moving the patient by gently ventilating and checking that there is no gas leakage and that the airway is patent.
The volatile agent should be turned off whilst the cause is investigated. The v-gel® size and position should be evaluated.
The most common reason for gas leaking would be under-insertion, either initially or due to movement during the anaesthetic. Confirmation of initial positioning should be carried out according to the Instruction for Use. Movement may occur if the v-gel® is not secured properly and/or the circuit is not supported, thus pulling the v-gel® rostrally.
Pre- oxygenation before induction is ideal, but not always tolerated by veterinary patients. However, oxygenation to ALL patients, (not just limited to brachycephalic and rabbits), can by administered with a facemask after initial induction and before placement of an airway device, often whilst waiting for a surgical plane of anaesthesia to be achieved. This technique increases the body’s oxygen stores, primarily in the functional residual capacity (FRC) of the lungs. A short administration of 100% oxygen before any airway management device is placed, prolongs the time to onset of arterial hypoxemia. This can be useful if the device placement is delayed due to any unforeseen circumstances
The tip of the v-gel® locates itself in the upper oesophagus, which provides additional protection against reflux material reaching the airway.
The dog v-gel® has secondary channel exiting out into the oesophageal tip allowing for the draining of reflux material. A gastric tube can be inserted into this channel to actively suction out material.
v-gel® Advanced devices have no metal parts, so they can be safely used in MRI/CT machines.
Assisted ventilation (manual and mechanical) have been used very successfully with cats and rabbits. However, due to the enormous range of head shapes and sizes in dog breeds and cross breeds, it is impossible to gain high pressure gas seal in every patient, with the limited number of v-gel® sizes currently available.
Following the size guide provided by Docsinnovent, a safe gas seal for spontaneously breathing patients is possible in most situations.
Manually assisted breathing and mechanical ventilators can be used, at the discretion of the clinician, only where a good seal pressure is achieved. A manometer measurement or held manual IPPV breath, to test seal, should be carried out prior to the use of continued regular ventilation. Auscultation of lungs and stomach should be monitored. The ventilator setting should not be higher than the seal pressure achieved with the device.
If a procedure is longer than 4 hours, the v-gel® should be removed with the patient placed on oxygen face-mask for 30-60 secs, before being replaced.
There are many published papers on the incidence of both reflux and regurgitation.
In dogs, reported incidence of reflux is over 70% in dogs (Raptopolous 2019, Rodriguez-Alarcon et al 2015) and 33.3% in cats (Garcia et al 2017)
The incidence of regurgitation is up to 48% in dogs (Viskier and Sjöström 2017), leading to aspiration in 0.17% (Ovbey et al. 2014)
The v-gel® devices have low dead space connectors fitted. However, it is impossible to simultaneously widen the airway and decrease dead space. At normal fresh gas flow rates this change is clinically insignificant. Docsinnovent’s veterinary consultants have not found clinically significant rebreathing to occur using the v-gel® and most clinicians agree that airway diameter is the most important thing to optimise ventilation for small patients.
The v-gel ® will be the best airway management device in most procedures involving the oral cavity, but there are limitations: There is obviously visibility and accessibility restrictions in the oral cavity when the v-gel ® is in situ: this will restrict the usage during major oral or pharyngeal procedures. It is also not possible to place a gastroscope whilst the v-gel® is in situ.
The simple answer is NO.
However, Docsinnovent advocates excellent standards of patient monitoring for the delivery of safe anaesthesia. During any anaesthetic procedure it is necessary to ensure that a patient’s ventilation is adequately maintained and monitored. There are several methods of doing this including:
– Observation of thoracic wall movement or observation of breathing bag movement when thoracic wall movement cannot be assessed.
– Auscultation of breath sounds with an external stethoscope, an oesophageal stethoscope, or an audible respiratory monitor.
– Capnometer (end-expired CO2 measurement)
– Arterial blood gas analysis for partial pressure of CO2 (PaCO2)
– Respirometry (tidal volume measurement)
If the patient is being monitored with at least two of the above in combination, then it is possible to safely monitor the patient where capnography is not available.
Both oesophageal stethoscopes and temperature probes can be used with v-gel® devices, however this can be difficult in very small patients.
The best way to use them is by placing the probe first followed by the v-gel®, which should lie ventral to the probe. In the Dog v-gel®, an oesophageal stethoscope or temperature probe can be inserted down the gastric channel (12fr)
All v-gels® are made from recyclable materials. Local rules should be followed for disposal of clinical waste.
The short answer is NO!!
This common association, especially when used in published papers either referring to the v-gel® as LMA® or incorrectly referencing other papers whereby an LMA® brand is used, is factually incorrect and very frustrating for us!
So why are they different?
LMA® is a trade name of a product invented by Archie Brain in 1988. There are now many different types of human-specific LMA® (eg Classic, Proseal, Flexible) available to the human anaesthetists, but it’s typically the Classic LMA® that has been previously used in some veterinary studies on dogs, pigs and rabbits but, due to them being human-specific, these have had limited success.
The v-gel® and the LMA® both come under the title of Supraglottic Airway Devices (SGAD), used to maintain airway patency by sitting outside of the trachea, above glottis, but they are very different in how they sit and create this seal.
As an early SGAD, the classic LMA® is a first-generation human device: a simple, low pressure pharyngeal seal with limited protection from aspiration and no specific design to lessen risk.
The device is essentially a soft diaphragm with an inflatable balloon around the edge attached to a tube. The diaphragm is inserted into the pharynx and the balloon inflated against the pharyngeal wall.
Over time and as things developed, second-generation human devices were bought to market: specially designed for more safety with a high-pressure seal coping better with patient ventilation and reducing risk of aspiration. These second-generation devices are more indicated for
- GA maintenance in shorter length procedures
- CPR to secure airway
- Essential pert of difficult airway trolley
- Primary device when urgent airway required
Within this second-generation group lays the i-gel®, invented by Dr Mohammed Nasir who goes on to develop the specie-specific v-gel® which was classified within the same grouping.
The i-gel® had many improvements on the Classic LMA®:an anatomically shaped device meant the negation of any inflation, sitting directly over the glottis mirroring the anatomical shape. Plus, the inclusion of an upper oesophageal seal with an integral gastric channel meant in all, there was less trauma and better protection and control of aspiration.
These same safety features were transferred to the original v-gel® (developed 2012 for cat and rabbit) with them being specie-specific i.e. anatomically correct for each species the device was intended for. The cat version did have an inflatable dorsal section to allow a higher seal pressure required for positive pressure ventilation. They protected the airway from aspiration by sealing in the upper oesophagus, but the gastric channel was only viable in the dog version (developed 2022) due to physical size of the devices.
In 2020 & ‘22 the improved v-gel® Advanced for cats and rabbits and the addition of the Dog v-gel® respectively, gave us essentially a third-generation device. These devices gave an increased seal pressure by now re-lining the whole pharynx containing the glottis inside the bowl, rather than sitting half-way down directly over the glottis and the dog device as previously mentioned had an integral gastric channel.
So, to directly compare a v-gel® Advanced to a Classic LMA® is like comparing a 1980’s Mini to a 2022 Jaguar. They are both cars, but different manufacturers and a totally different class in regard to safety features and comfort.